
Coronavirus fear is mounting as the mainstream media reports increasingly alarming statistics about the spread of COVID 19. As Italy becomes the global epicentre of the pandemic declared by the World Health Organisation we need to be extremely clear about what we do and do not know.
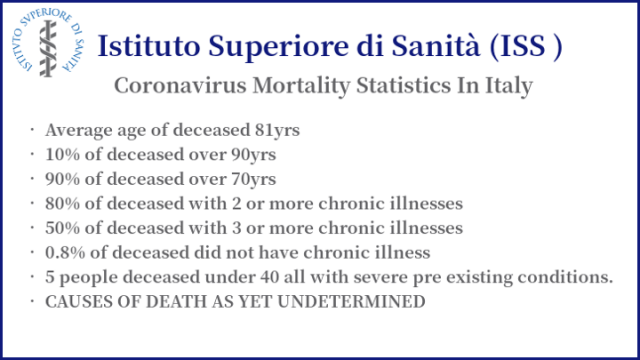
For example, while excess deaths in Italy appear to be alarming, according to the Italian Institute of Health (Istituto Superiore di Sanità -ISS), not only are 99.2% of reported coronavirus fatalities found in the most vulnerable of all patient groups but, while the ISS calls these “COVID 19 positive deaths,” it hasn’t actually determined if their cause of death was due to coronavirus or their pre-existing conditions. This doesn’t mean we shouldn’t be concerned but it does suggest reason for scepticism regarding the widely propagated statistics alarming so many.
Similarly in the UK, according to the government’s Chief Scientific Adviser Sir Patrick Vallance, with an estimated 540,000 deaths annually in England and Wales, and at least 20,000 “excess” deaths every winter, currently there is an unknown degree of “overlap” between reported coronavirus deaths and quite normal excess mortality. In other words, we don’t know if these deaths are unusual.
With the coronavirus outbreak now seemingly under control in China, we certainly shouldn’t simply dismiss early research which suggests the Infection Fatality Ratio for coronavirus in China was closer to 0.04% rather than the frequently reported death rate of around 4%. Though very basic maths should tell you that 3,242 deaths in a country of approximately 1.4 billion people, while unwelcome, are not statistically significant.
Given this, quite why the UK government assessment that 20,000 deaths (six times higher than China’s) in a population of just under 68 million people (on twentieth of the size of China’s) would prove how effective government response measures are is difficult to understand. With 20,000 excess deaths typically expected in the UK, presumably the government mean an additional 20,000 excess deaths. We will have to wait to compare the annual figures before any kind of meaningful assessment of the “overlap” can possibly be made.
None of these facts have stopped the mainstream media (MSM) reporting every death as if it proves reason for alarm. Consider how you would respond if the MSM reported every one of the quite normal 20,000 or so excess deaths every winter in the UK.
Awash with statistical claims and wild speculation about severity, we need to be learn new terms rapidly if we are to have any hope of understanding the information we are given. While we are all now familiar with the meaning of “self isolate” and “social distancing” how many of us know the difference between Infection Fatality Ratio (IFR) and Case Fatality Ratio (CFR)? I certainly didn’t until recently.
IFR is the number of deaths, as a percentage, based upon the number of known, projected or estimated infections. Projected infections are calculated from available data. CFR is the death rate relative to diagnosed cases and this ratio is often far higher than for projected numbers of infections. This differentiation was clarified by Sir Patrick Vallance who stated:
“There are currently 590 cases that have been identified in the UK and there are more than 20 patients in intensive care units……If you calculate what that really means in terms of the total number, it is much more likely that we have between 5,000 and 10,000 people infected at the moment.”
If we take Sir Patrick’s projections and margin of error into account this means, at the lower end of his estimate, approximately 10 times as many people have coronavirus than diagnosed. Currently the WHO are reporting 35,713 cases and 2,978 deaths in Italy. Seemingly a very alarming CFR death rate of over 8.3%. However, if we consider the likely IFR that death rate, though still concerning, conservatively drops to 0.83%.
Believing you have nearly a 1 in 12 chance of dying compared to nearly a 99.2% chance of surviving will make a considerable difference to your stress levels. Stress itself being extremely bad for your health. Particularly if you have underlying health conditions.

We Need To Talk About Chloroquine

States around the world insist that they are doing all they can to protect the public and limit the spread of the coronavirus infection. However, given the alleged severity of the declared pandemic, there are significant questions that need to be asked.
Chloroquine has emerged as both possible preventative prophylactic and successful treatment for the COVID 19 coronavirus. The evidence suggesting this possibility has been available for more than a month.
Chloroquine is an off patent generic medicine, used widely around the world as an antimalarial medication. It is cheap, easy to manufacture and plentiful. Repurposing or “repositioning” it, potentially for use in the prevention and treatment of coronavirus, could be done very quickly. Chloroquine, especially hydroxychloroquine in combination with azithromycin, if widely utilised, seemingly has the potential to limit both the spread and the severity of the coronavirus pandemic.
In light of the timeline below, we must ask what our governments are doing about repurposing trials of chloroquine for coronavirus treatment? Why has it taking them so long to react and, if further repurposing trials are necessary, when are they going to get on with them and widely distribute chloroquine? Initially to the most vulnerable who are medically able to take it.
The Chloroquine Coronavirus Timeline
- Februray 18th: – Japanese researchers publish encouraging initial chloroquine results
- February 19th/20th: – Chinese researchers publish results from clinical trials of chloroquine which identified it as the best treatment and a possible preventative measure against the onset of COVID 19. The Chinese researchers included full links to their data sets in their research which was immediately available to the global scientific community.
- 24th February: – Professor Didier Raoult, undoubtedly one of the worlds leading experts in infectious diseases, makes it clear that he considers chloroquine likely to be an effective treatment for COVID 19 coronavirus.
- 26th February: – An article appears where Prof. Raoult expands on his conviction about the effectiveness of chloroquine and states his confidence in the Chinese clinical trial results.
- 26th February: – The UK government bans all parallel exports of choroquine, suggesting they know about it’s treatment potential following publication of the Chinese clinical trial results.
- 3rd March: – The UK government publish their action plan. It makes little comment on potential preventative treatments, instead focusing heavily on development of a vaccine. Unlike the potential of chloroquine to impact immediately, the prospect of a future vaccine does nothing to prevent the current spread or severity of the outbreak. At this stage the Chinese clinical trial results and the Japanese research has been available for more than two weeks.
- 13th March: – Standford University issue a report called “An Effective Treatment For COVID 19.” They report not only the 4 week old Chinese clinical trial results but also acknowledge that in both China and South Korea they have been successfully treating COVID 19 patients with chloroquine. The Chinese and Koreans have adopted it as part of an apparently successful treatment protocol. While other governments around the world have yet to trial it. This accompanies the publication of Prof. Raoult’s own clinical trials of chloroquine. Though only a small scale study, reporting a 100% treatment success rate, the researchers conclude, “hydroxychloroquine treatment is significantly associated with viral load reduction/disappearance in COVID-19 patients and its effect is reinforced by azithromycin.” These findings largely replicate those of the Chinese clinical trials published on the 19th February.
- 13th March: – The UK Prime Minister Boris Johnson tells the British public that “..many more families are going to lose loved ones before their time.” Accompanying Johnson at the press conference, neither the UK government’s Chief Medical Officer nor the Chief Scientific Adviser give any indication of the reasons for hope. Again the focus of information sharing and advice is almost exclusively on passing responsibility to manage the outbreak to the public, telling them to “self isolate,” and the development of a future vaccine which does nothing to tackle the current spread or severity of coronavirus.
- 14th March: – In a truly bizarre decisions, despite all the scientific evidence, clinical trials and treatment success, the French health authorities rule out even trialling chloroquine.
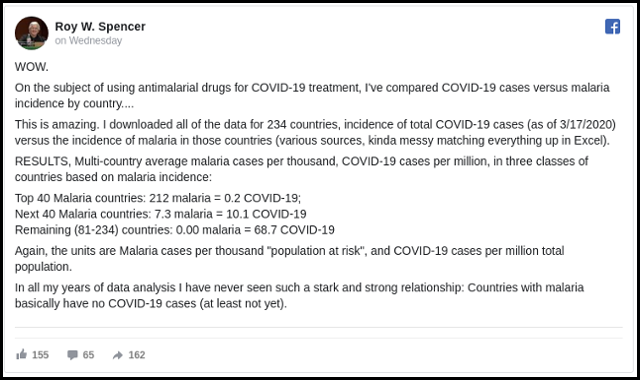
- 18th March: – NASA scientist Roy Spencer conducts a statistical analysis of COVID 19 coronavirus global distribution. He finds a direct inverse correlation between countries with high rates of malaria and coronavirus infections. The more malaria the less coronavirus. This again indicates chloroquine as a possible prophylactic preventative against coronavirus. It is in countries where malaria is most prevalent that chloroquine is most widely used.
- 19th March: – One month after publication of the Chinese clinical trial results, in the wake of President Trump’s acknowledgement that choloroquine is a potential treatment for coronavirus, the UK government announce that clinical trials of a vaccine could begin within a month. As yet the UK government have made no statement about the availability of chloroquine despite pharmacies reporting they have run out following the U.S. President’s comments.

Regarding the attitude of the French authorities (as well as mainstream media) towards chloroquine, explanations have emerged over the past week (or rather a series of scandals are emerging).
Pr. Raoult has a very influential old enemy: Yves Levy. He’s an eminent specialist of HIV, and the former head of INSERM, which is the rival research institute to Raoult’s IHU, with many ties to Big Pharma. INSERM is leading the French arm of the EU covid-19 clinical trials (Dicovery) which focus mainly on Kaletra (Abbot/Abbvie labs) and Remdesivir (Gilead labs), and which until last Friday completely excluded chloroquine.
Yves Levy is also the husband of Agnès Buzyn, who has been France’s Health Minister until Feb 16th of this year. On Jan 13th Minister Buzyn had chloroquine, until then an over the counter medicine, re-classified as a dangerous substance. At the same time, a massive media campaign was launched against Raoult (which continues to this day) calling him a charlatan, a climate denier, etc, and of course chloroquine had become a lethal drug. The so-called fact-checking team of Le Monde (Decodex) even qualified Raoult’s theories as “fake news” which caused his videos to be banned on Facebook. Among the most vicious attackers against Raoult in the media, there are prominent infectious diseases researchers at INSERM (like Karine Lacombe), who also happen have financial ties to either Gilead or Abbvie, or both.
Anyway, after a vote Raoult’s intitute decided last weekend to treat every covid-19 patient in Marseille with chloroquine (combined with an antibiotic), and to test as many people as possible and immediately treat the positive cases. We should see the result by next Monday.
Oh btw, in 2017 Yves Levy, along with the French PM, inaugurated the new French-built and accredited BSL-4 lab in Wuhan (modeled after the INSERM BSL-4 lab in Lyon). It doesn’t mean he’s in any way involved in the pandemic, but it’s rather curious to find him at both ends of the events, so to speak.
Thanks very much that is interesting information. I will look into it. However, in the meantime, could you please share any relevant links to the evidence supporting what you are saying. All the best.
Hi Ian
I’m afraid the links are in French, but you should get a decent translation from DeepL or Google’s sausage machine. Much of the rest is on twitter (just try “raoult” or “buzyn”, you’ll get a sense of what’s going on). Hope this helps.
Le Monde’s “fact checking” outfit’s page. They since have sort of walked back their accusations against Raoult, but a quick parse of their headlines should give you the picture:
https://www.lemonde.fr/les-decodeurs/
Wuhan BSL-4 lab inauguration:
https://cn.ambafrance.org/Voyage-officiel-du-Premier-Ministre-en-Chine-visite-du
Discovery clinical trials to include chloroquine, and description of protocols:
https://www.lesechos.fr/idees-debats/sciences-prospective/exclusif-coronavirus-le-gouvernement-confirme-le-lancement-dun-essai-clinique-de-grande-ampleur-de-la-chloroquine-1187599#xtor=CS1-26
All covid-19 patients at Marseille’s IHU to be treated with chloroquine:
https://www.francebleu.fr/infos/sante-sciences/coronavirus-la-chloroquine-propose-a-tous-les-malades-de-l-ihu-marseille-infection-1584895613
Hydrochloroquine classified as a poisonous substance:
https://www.legifrance.gouv.fr/affichTexte.do?cidTexte=JORFTEXT000041400024&categorieLien=id
The IHU-INSERM conflict:
https://www.marianne.net/politique/comment-matignon-tente-de-sortir-la-ministre-agnes-buzyn-d-un-embarrassant-conflit-d
Critics of Pr Raoult & their conflicts of interests:
Karine Lacombe:
Her declarations on French TV: https://twitter.com/infofrance2/status/1242061179012464642
Her declared links to Big Pharma:
https://cns.sante.fr/wp-content/uploads/2017/07/dpi_lacombe-karine_2016.pdf
https://aasldpubs.onlinelibrary.wiley.com/doi/full/10.1002/hep.29062
Francois Xavier Lescure (same sort of declarations on TV):
https://www.transparence.sante.gouv.fr/flow/rechercheBeneficiaires?execution=e2s9
Many thanks that’s a fantastic help. Much appreciated.