
In Part 1 we looked at the reasons why questioning the coronavirus lockdown, despite the ever present allegation, does not demonstrate a callous disregard for human life. We are going to expand on why it doesn’t in this article.
I am based in the UK so much of this discussion relates to the decisions of the British State, but this is a global policy agenda and similar policies are found across the developed world. Effectively a small group of policy decision makers have placed an estimated 3.5 billion people under house arrest. It is only possible for them to do so with our consent. Consent is carefully cultivated by controlling the information we are given.
 For the vast majority their only source of information is the corporate mainstream media (MSM) and the public announcements of the State. This article is written, as ever, in the hope people will do their own research and make up their own minds.
For the vast majority their only source of information is the corporate mainstream media (MSM) and the public announcements of the State. This article is written, as ever, in the hope people will do their own research and make up their own minds.
We are going to look at the evidence which strongly suggests the State and the MSM, adhering to a globalist agenda, have colluded to mislead the public into believing the COVID 19 (C19) threat is far greater than it actually is. C19 can be fatal for those with pre-existing comorbidities, and possibly even some without, as can other forms of pneumonia and influenza like respiratory illness. However, while every C19 death has been reported, none of the far greater number of people who have died in the UK this year from other respiratory infections have even been mentioned.
Systems have been created to ensure the C19 statistics are as terrifying as possible. Their statistical product is so vague it borders upon meaningless. It seems we have been inculcated with misplaced fear to justify the lockdown regime, to convince us to accept it and prepare us for what is to come.
I apologise for the article’s length but I hope you will read it in its entirety. There’s a lot of ground to cover, so please grab a coffee before we begin.
Lockdown Advised By WHO?
The World Health Organisation (WHO) is financed through a combination of assessed and voluntary contributions. Assessed contributions are paid by nation states for WHO membership and figures are released quarterly. Voluntary contributions are additional contributions from member states and “other partners.” For some reason these figures haven’t been reported for more than three years. About 80% of the WHO’s finances come from voluntary contributions.
In its most recent 2017 voluntary contribution report the WHO accounted for the $2.1 billion it received from private foundations and global corporations. This compared to just over $1 billion voluntarily provided by governments. Contributors included GlaxoSmithKline, Bayer AG, Sanofi, Merck and Gilead Sciences whose drug remdesivir is currently being trialled, along side the off patent hydroxychloroquine, as a possible preventative treatment for COVID 19. The remdesivir trial is part of the WHO’s SOLIDARITY trials.
 The third largest single contributor in 2017 was GAVI. Formerly called the Global Alliance for Vaccines and Immunization, they contributed nearly $134 million. GAVI are partnered with the WHO, UNICEF, the Bill & Melinda Gates Foundation and the World Bank to sell vaccines globally. The World Bank contributed nearly $146 million themselves and the largest individual payment, by some margin, at nearly $325 million came from the Bill & Melinda Gates Foundation (BMGF). Though like many other foundations and corporations, through their various networks of interlinked partnerships, their overall contribution was much higher.
The third largest single contributor in 2017 was GAVI. Formerly called the Global Alliance for Vaccines and Immunization, they contributed nearly $134 million. GAVI are partnered with the WHO, UNICEF, the Bill & Melinda Gates Foundation and the World Bank to sell vaccines globally. The World Bank contributed nearly $146 million themselves and the largest individual payment, by some margin, at nearly $325 million came from the Bill & Melinda Gates Foundation (BMGF). Though like many other foundations and corporations, through their various networks of interlinked partnerships, their overall contribution was much higher.
Among other beneficiaries of the BMGF’s generosity are the Vaccine Impact Modelling Consortium (VIMC) led by Professor Neil Ferguson. They are based at Imperial College London and are directly funded by the BMGF and GAVI. Their objective is to provide statistical data analysis for the BMGF and GAVI in order for them to sell more vaccines. Prof. Ferguson not only led the team who created the hopelessly inaccurate prediction which the U.S and UK governments based their lockdown regimes upon, he also co-founded the MRC Centre for Outbreak Analysis and Modelling who worked with the WHO in 2009 to create ridiculous computer models predicting the H1N1 pandemic.
In 2009 the world went crazy after the WHO declared the H1N1 influenza pandemic. This resulted in billions being spent on very expensive H1N1 vaccines and antiviral treatments although it turned out the pandemic was indistinguishable from seasonal flu. The only people who benefited from pointless vaccines and unnecessary medication were the manufacturers GlaxoSmithKline, Roche and Novartis. Each of these pharmaceutical corporations were among the largest voluntary contributors to the WHO in 2008/2009 financial year.
With an $84 million investment, the Swiss pharmaceutical giant Roche were the largest single contributor into the WHO’s coffers that year. Luckily, as it turned out, they could afford it because sales of their unnecessary Tamiflu H1N1 medication rocketed to more than £3 billion following the WHO’s declared H1N1 pandemic. Which was just a coincidence.
The whole debacle resulted in the Parliamentary Assembly of the Council of Europe (PACE) lunching an investigation into the WHO to look into the issue of a “falsified pandemic.” During the subsequent hearing the epidemiologist Dr Wolfgang Wobarg said:
“The WHO basically held the trigger for the pandemic preparedness plans, they had a key role to play in deciding on the pandemic. Around 18 billion dollars was spent on this pandemic worldwide. Millions were vaccinated for no good reason. It is not even clear that the vaccine had a positive effect, because it was not clinically tested.”
At the same hearing Professor Dr Ulrich Keil, Director of the WHO Collaborating Centre for Epidemiology at the University of Munster, said:
“A number of scientists and others are questioning the decision of the WHO to declare an international pandemic. The H1N1 virus is not a new virus, but has been known to us for decades…..In Germany, about 10,000 deaths are attributed to seasonal ‘flu, especially among older and frail people. Only a very small number of deaths, namely 187, can be attributed to the H1N1 virus in Germany – and many of those are dubious.”

Of course nothing came of it because PACE were making allegations against the World Health Organisation. The WHO don’t break the rules, they make the rules. Amazingly, probably because no one ever learns anything from history, we all believed the WHO this time.
To imagine these huge investments made by pharmaceutical corporations and private foundations don’t buy influence is so naive it barely warrants mention. The WHO is essentially a policy lobby group for the powerful globalists who own it. Why an organisation with such significant and clear conflicts of financial interests should be considered a global health authority is anyone’s guess.
On the 11th March the WHO declared the SARS-CoV-2 global pandemic. On 15th March 2020 UK Health Secretary Matt Hancock stated that vulnerable people would be required to quarantine themselves or self isolate. The State issued a set of guidelines for avoiding the spread of infection. On the 16th March UK Prime Minister Boris Johnson issued a statement advising people to practice social distancing, avoid non essential travel and warned that drastic measures may be needed to protect the NHS and the most vulnerable.
On the 18th of March the Director General of the BMGF funded WHO Dr. Tedros Adhanom Ghebreyesus gave a virtual press conference. He stated:
“WHO continues to call on all countries to implement a comprehensive approach with the aim of slowing down transmission and flattening the curve. This approach is saving lives and buying time for the development of vaccines and treatments. As you know, the first vaccine trial has begun……This virus is presenting us with an unprecedented threat”
We are about to discuss why COVID 19 is not an unprecedented threat. On the 20th of March Boris Johnson ordered the closure of all venues for social gathering, such as pubs, cafes and restaurants. On March 23rd the UK State legislated for the Coronavirus Act and placed the UK in lockdown. Just as the WHO and their other partners called on them to do.
Lockdown To Protect the NHS
The NHS was created to protect us, that’s why we pay for it. It is difficult to pinpoint exactly when this relationship flipped on its head. After years of chronic under funding by successive governments of all persuasions, interminable mismanagement, savage ideologically driven austerity cuts, crippling Private Finance Initiative debts and increasing privatisation for corporate profit, there is absolutely no reason to believe the State cares about either our health or the NHS. Every single major health policy and legislative decision, made over the last few decades, clearly demonstrates that it doesn’t.
The basic premise, apparently believed by so many, that the State has now decided to act to keep us safe is tragically comical. For us to swallow this tripe we need to be sufficiently terrified to willingly accept the imagined protection of the State. The MSM has been doing its best to make sure we are and that we do. The 24 hour fear-porn cycle is a wonder to behold.

Most of this is based upon claims about deaths and stories about desperately overloaded hospitals struggling to cope with the pressure. Meanwhile, as millions of British people remain under house arrest, glued to their TV’s and fondle pads, the data that has been released by official sources doesn’t back up any of the tales we have been spun. This inconvenient truth has been reported by very few in the MSM print media and has been met with deafening silence on our TV’s. Rather, the data has been convincingly spun to tell a story that doesn’t stand up to scrutiny.
Evidence of NHS overload is entirely absent. The State will claim this is thanks to the lockdown regime. Certainly the fact that people with other serious conditions haven’t been treated has alleviated pressure on the NHS. Unfortunately, the evidence also indicates the lockdown regime is probably killing them in increasing numbers. Though it seems unlikely the State will claim responsibility for that.
The Financial Times reported that close to half of the UK’s hospital beds were empty. With just 60% of acute beds occupied this is 30% less than this time last year. in the same period last year the NHS was creaking under the pressure of demand, prompting then Prime Minister Theresa May to suggest scrapping NHS targets. Once again, the State was only concerned with how the figures looked not about people dying on trolleys in corridors. This year it cares, honest!
During a supposed global pandemic we’ve had the lowest ever national A&E attendance. Manchester hospitals report a 57% bed occupation rate compared to their average of 94%. Most concerning is the huge drop in cardiology patients. With Heart disease killing more than 40,000 people under the age of 75 every year in the UK, and with a reported rise in fatalities last year, this prompted Professor John Howarth from North Cumbria Integrated Care NHS Foundation Trust to express grave concern.
“I am really worried that people are not seeking the help they need for important conditions other than Covid-19.”

Indeed, if your world view is supplied by the MSM, deaths from anything other than C19 seem to have become practically irrelevant in the space of a few weeks. The Health Service journal (HSJ) reports that the NHS has four times as many empty beds as normal. Confirming that more than 40% of acute beds are unoccupied. Even in London, the alleged epicentre of the C19 pandemic, that figure is still nearly 29%.
The much publicised Nightingale temporary hospitals, a mobilisation the MSM were keen to portray as putting the nation on a war footing, which were allegedly required to cope with the surge of C19 patients, aren’t necessary. Of the 1,555 Intensive Care Unit (ICU) beds available in London 1,245 are occupied. So questions must be asked why 19 patients, who presumably needed intensive care, were seemingly moved unnecessarily into the 4,000 bed London Nightingale over the Easter weekend.
Contrary to the claimed justification for the lockdown, as many have repeatedly warned, the health consequences of the lockdown regime could far outweigh the risks presented by C19. Excess mortality this year is higher than average but reported coronavirus deaths form a smaller part of that bigger picture.
The HSJ reported a senior NHS sources who stated:
“There could be some very serious unintended consequences. While there will be a lot of covid-19 fatalities, we could end up losing more ‘years of life’ because of fatalities relating to non-covid-19 health complications.”
The deputy director of research at the Nuffield Trust Sarah Scobie echoed this concern:
“The PHE [Public Health England] data suggests there could be significant problems already developing for heart disease related conditions patients, for example. Attendances relating to myocardial infarction at emergency departments have dropped right down, whereas ambulance calls in relation to chest pain have gone right up.”
Not only is there no evidence that the NHS is even close to struggling to cope with a non existent surge, the likely severe health consequences of the State’s lockdown policy are starting to emerge. When we look at the data on claimed COVID 19 deaths the picture only becomes more alarming.
Lockdown & Reported Deaths
Everyday, for weeks, the MSM has reported every single UK death which was supposedly due to COVID 19. This has been central to their effort to convince us of the severity of the pandemic. The reporting always supports the State’s narrative that the lockdown is necessary.
 Under normal circumstances, when someone dies, a person who knows them well, such as a family member, or someone who was physically close to the person at the time of death, is the qualified informant who can notify the registrar of the circumstances and non medical details of the death. That is not true for suspected C19 patients. A funeral director, who has almost certainly never met the deceased, can be the qualified informant. This places far more emphasis on the Medical Certificate of Cause of Death (MCCD) as registration can take place without any input from family or anyone else familiar with the circumstances of the death.
Under normal circumstances, when someone dies, a person who knows them well, such as a family member, or someone who was physically close to the person at the time of death, is the qualified informant who can notify the registrar of the circumstances and non medical details of the death. That is not true for suspected C19 patients. A funeral director, who has almost certainly never met the deceased, can be the qualified informant. This places far more emphasis on the Medical Certificate of Cause of Death (MCCD) as registration can take place without any input from family or anyone else familiar with the circumstances of the death.
Prior to the Coronavirus Act, the last attending doctor to the deceased had the responsibility to register the death. However, in the case of suspected C19 deaths, that duty can be discharged by a doctor who has never met the patient. The UK State guidance for C19 patients states:
“A doctor who attended the deceased during their last illness has a legal responsibility to complete a MCCD….. this duty may be discharged through another doctor who may complete an MCCD in an emergency period….In an emergency period, any doctor can complete the MCCD….For the purposes of the emergency period, the attendance may be in person, via video/visual consultation, but not audio (e.g. via telephone)….Where the certifying doctor has not seen the deceased before death they should delete the words last seen alive by me on.”
When an MCCD is completed the medical causes are listed sequentially with the immediate cause of death at the top and the underlying cause of death at the bottom of the list. For example, heart failure caused by pneumonia stemming from influenza would list the immediate cause of death as a heart attack and the underlying cause as influenza. That underlying cause is usually diagnosed through positive test results.
It is crucial to understand that for C19 to be recorded on the MCCD, as the underlying cause of death, there does not need to be any test based diagnosis of the syndrome. Diagnosis can simply be from observation of symptoms or CT scans. The guidance to medical practitioners states:
“if before death the patient had symptoms typical of COVID 19 infection, but the test result has not been received, it would be satisfactory to give ‘COVID-19’ as the cause of death, tick Box B and then share the test result when it becomes available. In the circumstances of there being no swab, it is satisfactory to apply clinical judgement.”
Given this seeming lack of clarity, guidance from the Royal College of Pathologists (RCP) is also concerning. In circumstances where C19 is merely believed to be a factor they advise that there is no need for a post mortem.
“If a death is believed to be due to confirmed COVID-19 infection, there is unlikely to be any need for a post-mortem examination to be conducted and the Medical Certificate of Cause of Death should be issued.”
Post-mortems are not standard procedure and are normally required only where the cause of death is unknown or where the circumstances appear suspicious. However, the recommendation of the RCP is another part of a systemic approach to C19 deaths which is inexplicably opaque.
Even when a sample test is undertaken to identify C19, questions remain. The RT-PCR test commonly used to test for C19 does not appear to be very reliable, nor is it designed as a diagnostic tool for identifying viruses. A study from the Department of Microbiology, Queen Mary Hospital, University of Hong Kong found wild variations in RT-PCR accuracy. It was found to be between 22% – 80% reliable depending on how it was applied. This general unreliability has been confirmed by other studies. Further studies show clear discrepancies between RT-PCR test results and clinical indication from CT scans.
Most of these studies indicate RT-PCR failure to detect C19 in symptomatic patients, so called false negative tests. When Chinese researchers from the Department of Epidemiology and Biostatistics School of Public Health conducted data analysis of the RT-PCR tests of asymptomatic patients they also found an 80% false positive rate.
Having passed peer review and publication the paper was subsequently withdrawn for what seem quite bizarre reasons. It was removed from the scientific literature because it “depended on theoretical deduction.” The paper was not testing an experimental hypothesis, it was an epidemiological analysis of the available statistical data. All such statistical analysis relies upon theoretical deduction. The claimed reason for withdrawal suggests that all data analysis is now considered to be completely useless.
It seems scientific claims that C19 numbers are underestimated are fine, claims they are overestimated are not. Either way, whether false negative or false positive, there is plenty of evidence to question the reliability of the RT-PCR test for diagnosing COVID 19.
The MSM has suggested that enhanced RT-PCR testing can detect the virus SARS-CoV-2 and, in particular, the amount of it in the patient’s system, the viral load. This is disinformation. The Nobel winning scientist who devised PCR, Karry Mullis, speaking about the use of PCR to detect HIV stated:
“Quantitative PCR is an oxymoron.’ PCR is intended to identify substances qualitatively, but by its very nature is unsuited for estimating numbers [viral load]…. These tests cannot detect free, infectious viruses at all……The tests can detect genetic sequences of viruses, but not viruses themselves.”
Reported C19 deaths can be registered without a test clearly diagnosing any coronavirus, let alone C19. The death can be signed off by a doctor who has never seen the patient and can then be registered by someone who has never met the deceased and was nowhere near them when they died. Further provision in the Coronavirus Act then allows for the body to be cremated, potentially against the family’s wishes, ensuring a confirmatory autopsy is impossible, though it is unlikely one will be conducted anyway.
To say this raises questions about the official reported statistics is an understatement. Questions in no way allege either medical malpractice or negligence. Neither are required for significant confusion to occur because the potential for widespread misreporting of causes of death seems to be a core element of the C19 MCCD process the State has constructed.
Lockdown the Data
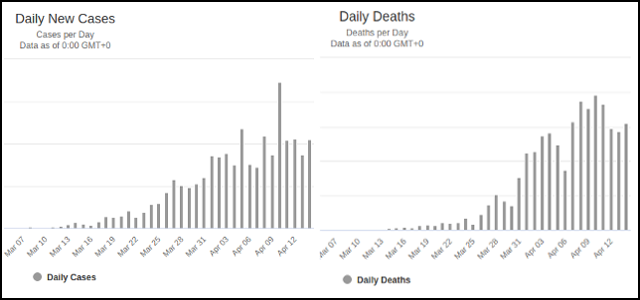
At the time of writing The UK is said to have 93,873 cases with 12,107 deaths attributed to C19. Both the infection and mortality rates are showing a declining trend. Given the apparent haphazard reliability of tests, strange reporting procedures and oddly relaxed registration requirements, the claimed attribution is pretty weak. Coupled with the data which shows unusually low hospital admissions, with little to no evidence of the widely anticipated “surge,” justification for the State’s lockdown of society and the economy appears painfully thin. The evidence base does not improve when we look at the official data.
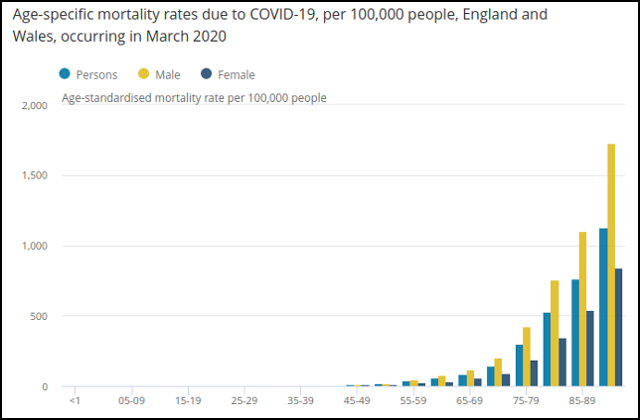
The Office of National Statistics (ONS) have released analysis of the C19 deaths that occurred during March 2020. In total 3,912 deaths were recorded of which 3,372 (86%) listed C19 as the underlying cause of death. Of these, 38 (1%) were cases where C19 was only suspected as the underlying cause, meaning neither a test nor any clear clinical presentation was observed. The problem is that the RT-PCR test, supposedly confirming C19, doesn’t tell us much either.
Of the 3,372 deaths recorded with underlying C19, approximately 3,068 had at least one comorbidity with the majority having more than two. Not only does the RT-PCR test fail to provide any reliable proof that these people even had C19 the existence of other comorbidities provides further reason to question if the C19 was a contributory factor.
Of the 3,912 people who died, 540 of them merely mentioned C19 on the MCCG with no indication that it contributed to the deaths. With at least 91% of patients having comorbidities, there is very little evidence that the people who died with a C19 infection wouldn’t have died without. The age profile of the deceased is practically identical to standard all cause mortality in the UK. If C19 is a viral pandemic it is one that behaves like normal mortality. And yet, despite all this, the MSM reported every one of them to the public as confirmed C19 deaths.
Another, perhaps even more alarming possibility has arisen. While heart disease accounts for 14% of C19 comorbidities, reported deaths from heart disease have mysteriously dropped by the corresponding amount during the same period. This clearly indicates that patients dying from other causes, such as heart failure, are being recorded, and certainly reported by the MSM, as dying from C19.
This illustrates a far more complex picture than we have been given to believe. Why have the State and the MSM made so many alarming claims about people dying from C19 when the evidence supporting those claims is, at best, questionable?
None of this is the fault of medical practitioners or bodies like the Office Of National Statistics (ONS). The ONS system has been both reliable and informative for many years. Yet once again, in the case of C19 deaths, the State felt it was necessary to make some changes. On the March 30th the MSM reported that the UK State had instructed the ONS to change the way they record C19 deaths. Explaining the change to recording “mentions” of COVID 19 an unnamed spokesperson for the ONS said:
“It will be based on mentions of Covid-19 on death certificates. It will include suspected cases of Covid-19 where someone has not been tested positive for Covid-19.”
 This habit of states deciding to change the C19 mortality data, by adding in people who are assumed to have died from it, appears to be a global policy. The China CDC did the same and the U.S have just added a significant number to their statistics. In every case the revision increases and never decreases the fatality statistics. Why do states around the world feel the need to do this? Is it because they are concerned about statistical rigour or are they more concerned about justifying their lockdown regimes?
This habit of states deciding to change the C19 mortality data, by adding in people who are assumed to have died from it, appears to be a global policy. The China CDC did the same and the U.S have just added a significant number to their statistics. In every case the revision increases and never decreases the fatality statistics. Why do states around the world feel the need to do this? Is it because they are concerned about statistical rigour or are they more concerned about justifying their lockdown regimes?
The ONS reported all cause mortality for week 14 ending April 3rd. They recorded 16,387 deaths which was 6,082 higher than the ONS 5 year average. They stated that 21.2% of total deaths “mentioned” Covid 19. The MSM immediately pounced on this claiming this meant COVID 19 had pushed up the death toll to unprecedented levels. This was outrageous disinformation. That is not what the data showed.
The ONS stated that of the 6,082 excess deaths 3,475 “mentioned” coronavirus. Of those 1,466 also mentioned influenza and pneumonia. Consequently, while registered deaths are 6,082 above the 5 year average, only 2009 of those solely mentioned C19 with 4,073 mentioning other underlying causes. It is worth remembering only C19 deaths can be “mentioned” without a clear positive test result.
Therefore, at least 67% of that excess mortality is being caused by other unknown factors that no one seems to care about. The MSM have absolutely no interests at all in this more severe health crisis. Why not? Once again they have completely misled the public and deny the existence of another, more significant reason for concern. Perhaps anticipating this the ONS stated:
“Influenza and Pneumonia” has been included for comparison, as a well-understood cause of death involving respiratory infection that is likely to have somewhat similar risk factors to COVID-19.”
Short of openly stating that C19 is no more deadly than any other pneumonia like illnesses, the ONS appear to be trying to get a message across. Perhaps they can’t say it directly.
As the so called pandemic has progressed more in depth studies have begun to emerge. Initial findings from Chinese scientists indicate that SARS-CoV-2 has an infection fatality rate (IFR) of between 0.04% and 0.12%. which is comparable to flu pandemics with an estimated IFR of 0.1%. None of these have required a lockdown regime. Further studies have highlighted the overestimated risk allegedly presented by SARS-CoV-2.
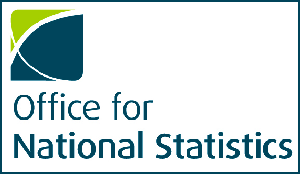
For the year to date, the ONS showed a comparison of the deaths mentioning C19 and deaths mentioning pneumonia and Influenza. Deaths this year from pneumonia and influenza appear to stand at around 30,000. Quite clearly, according to the ONS, other respiratory infections, like pneumonia and influenza, currently pose a significantly greater threat to life than COVID 19. Something is certainly pushing up mortality in the UK but, at the very most, only 33% of that increase is vaguely attributable to C19.
Lockdown To Cover A Myriad Of Sins
The MSM have recently started floating the idea that the lockdown regime could become the new normal. According to the State it may be necessary to go in an out of various levels of the regime from time to time, depending on the State’s threat assessment. This is based on scientific research bought and paid for by pharmaceutical corporations and private foundations including GlaxoSmithKline (Wellcome Trust).

Seeing as it is increasingly evident that the C19 threat has been massively over-hyped, why would the State and its globalist partners want the economic destruction to continue? Firstly it delivers on a number of long held globalist objectives. A cashless society, mandatory vaccination, universal basic income, a surveillance state, restricted freedom of movement and a complete restructuring of the global economy have already been touted as necessary following the “pandemic.” All of these ambitions and economic realities existed before the pandemic first emerged in China.
The State has already moved towards censoring anyone who questions vaccines. It is vital to understand that the canard of the antivaxxer is a meaningless trope. It is entirely possible to accept that vaccines can contribute towards effective preventative public health programs while, at the same time, questioning the efficacy and purpose of some vaccines. Vaccines are not all the same. The State’s and the MSM’s insistence that anyone who question any vaccines is some sort of whacked out, new age, science Luddite is total nonsense. No one will be permitted to question vaccines, and that fact alone should be sufficient to raise anyone’s suspicion.
From GAVI to the WHO and from the BMGF to Imperial College the response to the C19 pandemic has been driven by foundations and pharmaceutical corporations with considerable investments in vaccine development. Of course they would like to see global mandatory vaccination. To just ignore this, because you’ve been told by the MSM that questioning any vaccine is a “conspiracy theory”, not only evidences a lack of critical thinking it demonstrates a degree of brainwashing.
Global financial institutions, such as the IMF, have been advocating the cashless society for years. A cashless society will allow central banks to control every aspect of your life. Everything you buy can be tracked and your purchases could easily be limited to exclude certain items. Although there is very little evidence that handling cash presents any increased threat of infection that hasn’t stopped the MSM from selling the idea.
The impact of the lockdown regime across the globe has already had a devastating economic impact. All the indicators are that the regime will throw the global economy into a deep depression. The longer it continues the worse it will get. The tendency of some to claim this doesn’t matter because saving life is the only concern is hopelessly myopic. The link between poverty and significantly increased mortality is beyond dispute. The cure will definitely be far worse than the disease.
As millions are forced into unemployment the outlook isn’t good. However, while the State will undoubtedly claim that unemployment has been caused by the C19 crisis, in truth the imminent economic collapse was already driving up unemployment before the crisis began. This has led to increasing calls for the State to provide a Universal Basic Income. This will create mass dependency upon the State for huge swathes of the population. Affording the State immeasurable control over people’s lives. In a cashless society, people who don’t behave in accordance with State regulations, could be punished financially. Instant fines will be commonplace.
We are already seeing how that control can be deployed within a surveillance society as the State and its compliant MSM put the idea of immunity passports into the public imagination. The link between this and mandatory vaccination is obvious. This proposed policy comes straight from the heart of the globalist think tanks.
ID2020 is a globalist initiative which intends to provide everyone on earth with an authorised identity. GAVI, Microsoft, BMGF and the Rockerfeller Foundation are among the happy ID2020 alliance who will decide who you are allowed to be.
Comically they claim that proving who you are to the State is somehow a human right. This is utter bilge. I don’t know about you, but I know who I am and so do the people I care about. I couldn’t care less who the State thinks I am. Like everyone else on Earth you were born with inalienable human rights. The State doesn’t define what they are, they just choose to ignore them.
ID2020 is in no way objective. Your digital biometric ID can be “good” which means it can also be “bad.” Bill Gates and Rockerfellers are among those who state:
“With a “good” digital identity you can enjoy your rights to privacy, security, and choice.”
Which means you can’t if its “bad.” As longs as you are a good citizen, do as you are told, get your mandatory vaccinations and don’t step out of line, you can have your rights because megalomaniacs think they are gods who have the power to allow or deny them. Your digital ID will control the information you are allowed to access and your immunity passport will almost certainly be part of your State authorised identity as we move towards something indistinguishable from China’s social credit system. It will be used to monitor your behaviour.
Your immunity passport status will depend upon where you go and who with. The State has decided that we all need contact tracing apps to regulate who we meet and limit our freedom of movement. If you meet the wrong person or go to the wrong area, or perhaps fail to produce your authorisation Q-code on demand, then you will be locked down.
Perhaps the biggest deception of all is yet to come as the State manoeuvres to blame the C19 for the economic collapse. Firstly, it isn’t C19 but rather the lockdown regime that has sped up destruction of the economy, but that destruction was inevitable anyway. The 2008 credit crunch was a failure of the banks. They speculated in the markets and lost.
As a result we have endured a decade of austerity to bail them out. Socialism only applies to those who can afford it. Austerity has reduced essential public services to rubble, and now, when we supposedly need them most, we’ve all been placed under house arrest to stop us using them while many of the most vulnerable have been ignored. The irony is laughable.
While we’ve all suffered austerity, the central banks have been printing funny money, blowing up the debt bubble to unimaginable proportions. The result has been increasing consumer debt, staggering levels of corporate borrowing and, though government deficits have reduced, government debt is off the charts, even in comparison to 2010 levels. This kind of debt based economy was never sustainable and global financiers have known it for years.
What the globalists needed was a reason to reset the economy without losing power. Perhaps it is another coincidence that the C19 lockdown regime just happens to deliver both the mechanism and the excuse to press that global reset button. That it also ushers in all the globalist’s desires is just another in a very long line of remarkable coincidences.
Now that global terrorism is no longer a daily threat and global warming has been put on the back burner, the new normal of the ever shifting threat from pandemic seems to be the novel war on terror. Training, funding and equipping terrorist groups has served the State well in the first two decades of the 21st century but now it is ready to move on to the next phase by exploiting a terror closer to the heart of every home. Disease.
In their totality, for those willing to look, it is transparent that these response measures have coalesced to create the framework for a totalitarian dictatorship. One rolling out at pace in the UK. Similar draconian diktats have sprung up across the globe. A coordinated global effort like this doesn’t just happen. It takes years of training and planning. The only people who can’t see it are those who, for whatever reason, choose not to.


They know that we know that this pandemic is a phoney pretext for an authoritarian take over, and it doesn’t make a single bit of difference… But if we all stood up and walked outside right now, this madness would end immediately.
Thanks Cameron. I couldn’t agree more. Our behavioural consent is key. If we don’t give it they’ve got nothing and can do nothing. However, I’m certainly not advocating ignoring the State’s fantastic lockdown policy. Like you, I’m a good citizen.
An excellent article as usual, thanks.
Thank you. Please share it far and wide. We need to get the information out.
Bravo, here here.
Mr Whitty & Mr Pollard are innocent either .
What did Whitty get from BMGF? $40 million? What’s the crack with Pollard then?
*not
An excellent article. However, I would like to speak to you about a possible error you made using the ONS statistics. Please reach out to me on my twitter @zcaboah
Thanks
Thanks. Yep just done that.
A big thank you to Zcaboah for their invaluable help on this article which has been revised after they pointed out some errors.
This is something I actively encourage all readers to do. If you spot errors or think I’ve miscalculated or misunderstood a key point please don’t hesitate and let me know. These are my opinions based upon the facts as I understand them but that doesn’t mean I’m right.
If anyone is interested in working collaboratively please leave a comment with your email. All comments are moderated and I will not share your email with anyone or post the comment with your email on it.
Once again, thanks Zcaboah.
Here, here. I always say the same thing. It’s so useful to have people that see errors – even if they are minor – everyone learns and the end product is all the better for it.
Once again Iain, great job.
Excellent article. A must read for all.
Many thanks. Please share it far and wide.
Just approaching 30 days of this “lockdown”.
I live alone in a one bedroom flat. Boredom set in a while back and now feeling a bit depressed. At this point, I have no idea where the money for rent/bills is coming from. I’m sure there are many like me.
And for what?
Likely a fabricated health scare, allied to the most astonishing display of hysteria I have ever witnessed. And it is global.
This is all about something entirely different and the implications are making me very nervous.
Thank you. Your article has demonstrated that not everyone has lost their marbles. Well argued.
You can go out for “essential” reasons. If you are familiar with these “essential” reasons and are stopped by the authorities, as long as you inform them that you are outside for one of these “essential” reasons they have no reason to stop you going about your business. So familiarity with the “essential” reasons is quite important.
Here are the “esential” reasons according to National Police Chiefs’ Council: https://thedailywake.com/2020/04/17/uk-police-chiefs-publish-list-of-acceptable-reasons-to-leave-home-during-coronavirus-lockdown-news/
I’m 76, have no underlying health conditions other than blackouts, which have been controlled and completely eliminated by small daily amounts of prescribed drugs for the past 6 years, and occasionally gout which is controlled (self diagnosis) by not drinking wine of any stripe at all.
For the past 5 years I have declined my GP’s kind offer of a “influenza jab” and in that time I can hand on heart say that I’ve not contracted so much as a common cold. This could transpire to be “commentator’s curse”, as they say in the horse racing world, or might my body be carrying something that is an active and effective deterrent to “bugs”? Other wrinklies are I’m sure in the same position. Would Government be at all interested in this apparent phenomenon?
It certainly would make an interesting study. Unfortunately Roger I don’t imagine for a second that any such study would ever get any funding. So no, I don’t think any government would be interested.
“Therefore, at least 67% of that excess mortality is being caused by other unknown factors that no one seems to care about.”
Yes indeed. Peter C. Gøtzsche recently booted out of Cochrane Collaboration – guess what he had something to say about vaccines – which he co-founded has said prescription drugs are the third major cause of death after cancer and heart disease. Why does this happen? Because almost no one has a cytochrome P450 gene test to establish their personal phenotype (the ability of your enzymes to activate and inactivate drugs, if you can not inactivate drugs you become toxic) of drug metabolising enzymes. It’s been around for over twenty years look up: BBC Made to measure medicine from 2000.
Thanks Chris, yes his comments were very interesting. Great comment with some excellent information.
As much as the “Theorists” will discuss all facts & statistics about any global changing event – It seems in this case – No one discusses actually having Covid19 affect them or their families.
Jumping on anyone’s back at this time is an easy way to say “Listen to ME”
Actually having this virus, feeling as though you’re drawing your last breath, watching your friends & family die who are infected, not being able to see them or mourn at their funeral, guilty thoughts of did I pass this to someone who died…
These are all completely avoided.
The article is one sided & tries to suggest we are all sheep following the MSM & there is a greater meaning to all this.
I’m not saying there isn’t – I’m talking from life experience, not stats or theories of who has what & will gain from this.
STAY HOME – HALT THE SPREAD, unless you feel the need to watch people close to you go through the Covid death throws – No conspiracy theory will ever take the images or feelings away from the truth I have witnessed.
Hi Tony so sorry to hear the stories about your terrible loss. My sincere condolences. I hope you didn’t think I was suggesting people disobey government orders. That wasn’t suggested in the article nor am I aware of suggesting anywhere else. Unlike you, I am relieved to say that I haven’t met anyone who has this terrible disease. Nor has anyone I know nor, to my knowledge, has anyone in my local community succumbed to its ravages, nor any of my former colleagues. Which is a relief, as many of them work in the NHS. Thankfully they tell me that everything is quiet and they have only had a few cases. We must have been very lucky here on the South coast. But I hear what you are saying loud and clear and strongly support the use of the precautionary principle. In fact there are a number of areas, such as the roll out of 5G and the lockdown, where I wonder why the precautionary principle doesn’t count.
Tony if you copy and paste this into YouTube you will see scientific evidence of what happened: Peter Breggin US and China Collaborated to Make a Deadly Coronavirus.
Peter Breggin might be a new name to yourself if so, I assure you he is massive, a real heavy weight at exposing the harms of prescription drugs in particular psychiatric drugs.
Remember our leaders saying we will be led by the science. I’ve studied at great detail how corrupt the ‘science’ has become. To date the general public do not wish to listen or know, but now it’s time because enormous amounts of people are going to be psychologically affected with significant disabling anxiety/depression as a result of this on going shock.
Also someone made this significant comment on the Breggin video:
“This research was funded by USAID (Agency for International Development, not allergy and infectious diseases), a long-time CIA front group as part of their global pandemic preparedness project USAID-EPT-PREDICT (see corrigendum in Nature publication). UNC and Wuhan Institute of Virology engineered this virus with gain of function to infect human airway cells via ACE2 receptor, the very mechanism Covid19 uses. I ran some analyses and this 2015 virus has around 80% sequence identity to Covid19. This means it could be a prototype or ancestor of Covid19”
The change ‘corrigendum’ can be found in the ‘change history’ of the paper. I’d really like to see this persons analyses.
Hi Tony, I don’t mean to be insensitive but if you’re comfortable to do so, could you please elaborate on your experience as I think that it could help give us a clearer picture. I have to ask, as if there is a highly dangerous virus out there then we should know about it from those affected, not those who stand to profit from those affected. I struggle to believe the official narrative due to the immense conflicts of interest involved and the statistics being manipulated to justify a lockdown, rather than a lockdown being justified by actual evidence. Still, I wouldn’t to throw the baby out with the bathwater and remain ignorant of people actually suffering. Many thanks for any info. 🙂
Good article but please dig deeper for your supporting documentation. Voluntary Contributions 2018 report released May 2019.
Further evidence for you. https://www.who.int/about/finances-accountability/reports/A72_INF5-en.pdf?ua=1
Many thanks Nico. Thanks for bringing it to my attention. I wonder why the WHO don’t list this on their main page for voluntary contributions.
https://www.who.int/about/finances-accountability/funding/voluntary-contributions/en/
Could you provide the WHO link to where it is listed please?
I note the GAVI alliance and the BMGF are the biggest contributors again.
Thank you for writing these articles Iain, unfortunately the people I know who are open to questioning the MSM narrative are few and far between, but should anyone express an interest your articles will be the first I recommend.
Thanks for the encouragement and please do share them with those interested.
Hi Mr Davis,
Can you comment on the lates ONS data on total deaths and explain the spike in total deaths?
https://www.ons.gov.uk/visualisations/dvc799/fig1/line/fallback.png
From the ONS website,
https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/bulletins/deathsregisteredweeklyinenglandandwalesprovisional/weekending10april2020#deaths-registered-by-week
I am asking just about total deaths and not about the provisional covid subset.
Does the spike in total deaths prove that there is something real happening and that therefore our self quarantine is justified or not in the current period?
Thanks DG for an excellent question. The figures are extremely concerning. What they show is that of the 7,996 above average all cause deaths in week 15 a total of 3880 solely mentioned C19 and 4116 were attributable to other causes or combinations of causes including C19. A notable massaging only of the C19 death statistics was also reported by the ONS and the comparison they made with other all cause mortality was notable. It certainly proves something real is happening as I have tried to highlight in this post. Mortality has increased significantly above the 5 year average. No it certainly doesn’t justify the lockdown in my view. Quite the opposite. I hope you read my next article where I will address this question in some detail.
I’m sorry I don’t quite follow – you agree something significant is the cause of the extra 6,000 to w/e 3/4 and 8,000 to w/e 10/4 – yet are saying they would not have been even higher without the quarantine! How does that work?
I note that the Financial Times has followed up with their calculations which claims that we may be at the 40,000 mark already!
https://www.ft.com/content/67e6a4ee-3d05-43bc-ba03-e239799fa6ab
Are they lying? Who to believe? When will we know for sure? Next week? Next month?
Thanks DG. What makes you think the mortality and infection rates would have been higher without the quarantine? Many countries have chosen not to implement a quarantine and with no notable, comparative detrimental effect on either infection rates or mortality. I will be covering this in more depth in my next post.
Well it seems mass quarantine is not the only weapon in the armoury of epidemic control is it?
It ought not to be a last ditch but part of effective measures depending on levels of infection rates.
Testing and tracing is a lot more effective if done early enough.
Hence Germany. Which did just that and is doing hundreds of thousands of tests while the UK can barely manage 10’s if thousands.
It is the clearest comparison for the layman to look at and avoid being misled by damn lying stats.
Thanks DG. Yes it is also notable that Germany had plenty of ICU capacity with 25,000 beds compared to the UK’s 4,000. So initial reasons for panic were less in Germany too.
Let me start with a joke:
There’s a guy walking down Main Street with a stick, loudly beating lantern posts.
Passers by alert the police about the commotion, who ask the guy what on earth he thinks he is doing?
The bloke replies: “I’m doing it to frighten off the elephants ”
Policeman: “But there are no elephants here”
Bloke: “See! It’s working”
“… only to find that the social distancing worked better than the projections indicated… That’s nobody’s fault, and it’s an unmitigated win”
This will be an endless refrain in the aftermath. Does the evidence support it?
NO.
Backdated (for incubation time [5 days] + symptom progression [7 days], before people will present with serious symptoms to get tested [12 days]) R₀ values show values were dropping before measures were announced, everywhere, in all jurisdictions.
Looking at the rate of increase in new cases is significant, and is not just an artefact of testing and is independent of variance between countries in terms of absolute numbers or comorbidities, cause of death protocols, etc, as long as they retain a consistent gateway protocol for doing a test. In most cases that applies. Every case I’ve looked at, the logarithmic curve (kind of a mild S shape or “logistical” curve) shows the kink in the bend to the second part of the S before NPI’s (non pharmaceutical interventions) could possibly have an effect [12 days; since the measures target the moment of infection, not the onset of symptoms]. The effect should show a definite step sometime around 12 days after instituting measures, since the measures take effect in a single step, and do not grow slowly. In every case, you see the curve starting to bend sometime BEFORE those 12 days and bending smoothly, meaning, as in Wuhan/China, something else is influencing transmission. That could well be dampening due to building (significant) herd immunity (or something else, who knows). Probably we will later discover that far more people are either sero-converted or insusceptible (or something else) than we think, dampening transmission rates, meaning we have captured the height of the wave, not the beginning.
Excellent article, well written and I agree 100% including the very likely corruptness of the WHO. To be honest, their officials always reminded me of FIFA. Not with you (yet?) on the Global conspiracy theory, but that may be partially because it scares me too much. Keep up the good work, Biffo.
Thanks Biffo. FIFA is an excellent analogy. In fact I think FIFA is a pretty good analogy for all globalist institutions. The globalist “conspiracy” is tricky because any mention of it leaves the impression that you believe the people involved are all powerful omnipotent beings. To be clear, that is what they believe about themselves not what I believe. The process of centralising power is as old as human history itself. If you want more information about the modern history of the New World Order please check this post out: https://iaindavis.com/who-are-the-new-world-order-a-brief-history/
Great job Iain.
I have question about the following statement(s):
“The Financial Times reported that close to half of the UK’s hospital beds were empty. With just 60% of acute beds occupied this is 30% less than this time last year.
During a supposed global pandemic we’ve had the lowest ever national A&E attendance. Manchester hospitals report a 57% bed occupation rate compared to their average of 94%”
Had a word with my housemate who’s sister works in a hospital in London – apparently they’re busier than usual? Same story from his sisters’ friend who works in a different hospital in London.
Is the situation with hospitals different in London? Any thoughts?
Cheers
Thanks Serge. I think London has been a “hot spot” and ICU capacity may well have been overwhelmed had they not increase the 750 or so ICU beds to more than 1550. They also built the Nightingale for extra ICU capacity though that hasn’t been needed. However, with the extra capacity, even at its peak, London still had 300 free ICU beds (not including the 4000 claimed Nightingale Beds.) So London, and I think Birmingham, were busy during this period. However, this picture is not replicated nationally yet the NHS has been closed to all but C19 care across the country.
This means that hundreds of thousands of people haven’t been treated for serious conditions for more than a month. Among them are cancer and heart patients. I too have family members who who work in the NHS, vulnerable people I care for and I worked in my local general hospital as a substance misuse counsellor for many years. During this alleged pandemic I heard from a consultant at my former work place who stated that the 1200 capacity general hospital had 500 empty beds and just 11 active C19 patients. At no time during my years of working there, nor since, prior to this alleged crisis, has there been any spare bed capacity at the hospital. It was constantly on “red bed alert.” Full in other words.
Replicate this picture across the nation and it seems clear to me the lockdown itself has created a coming health crisis signifiantly gretaer than the alleged C19 pandemic. Add to this rising deaths from all the morbidity associated with genuinely unprecedented levels of poverty, and we are looking at something far worse than COVID 19 I’m afraid.
hello my friend great post, please read this article i wrote on the govt foot and mouth scam. this will give you insight into my investigative style, and then do pls email me i am sure we’ll have lots to discuss! i’ve also nearly finished my c19 expose but need to know a bit more about ‘i’m lying coz my lips are moving chris whitty’, somebody mentioned he received 40 million from somewhere? bless you my fellow UK dissenter, here’s the linkhttp://www.karting.co.uk/News-FMArticle.html
Thanks Steven. I’ve removed your email address (for your security) and will email you shortly. Yes Witty received a $40M (£31M) in 2008 from BMGF for ressearch into Malaria. Also Patrick Vallance is the former head of R&D for GSK. He almost certainly still has a financial arrangement with them.
“At the time of writing The UK is said to have 93,873 cases with 12,107 deaths attributed to C19. Both the infection and mortality rates are showing a declining trend”
Should this not be updated? Has the near tripling of the reported number of deaths in the last month changed anything?
David you can’t perpetually update a post, based upon statistics, every time new statistics come out. It would never be an article just a list of never ending statistics. However I may well write another post in light of the alarming increase in mortality, especially from care homes. Clearly the number of excess deaths from everything but COVID 19 is very concerning as is the apparent policy of discharging COVID 19 patient to “isolate” in care homes.
Thank you Iain – relieved to have stumbled across your site. The silences and blank faces when i’d been saying (since January) that the virus was an excuse to blame for the collapsed economy had left me feeling lonely. But now i see that all this mess/ tyranny will have the great benefit of waking us all up to realising that we can assume our sovereignty.
I am still upset that NHS do not offer ill people any help until rather late. There are so many natural anti-virals and immune boosters which would help, eg. Andrographis paniculata, Artemisia, licorice, Boswellia, garlic, ginger, elderberry, eucalyptus, yarrow (Achillea millefolium), propolis, N-acetylcysteine (NAC), melatonin, glutathione, CDP Choline (aka Citicoline), UV light, infrared sauna, hydrogen peroxide, ozone, hydrogen, convalescent plasma.
I’m not a doctor, but there’s loads of evidence showing good efficacy of vitamin therapy.
eg. https://www.mdpi.com/2072-6643/12/4/1181 “Optimal Nutritional Status for a Well-Functioning Immune System Is an Important Factor to Protect against Viral Infections”
http://www.orthomolecular.org/resources/omns/v16n21.shtml “Rationale for Vitamin C Treatment of COVID-19 and Other Viruses”
http://www.orthomolecular.org/resources/omns/v16n25.shtml “Vitamin C Evidence for Treating Complications of COVID-19 and other Viral Infections”
http://www.orthomolecular.org/resources/omns/v16n27.shtml “Protected Group Immunity, Not a Vaccine, is the Way to Stop the COVID-19 Pandemic”
http://www.orthomolecular.org/resources/omns/v16n28.shtml “Vitamin C and Coronavirus: Not a Vaccine; Just a Humble Cure”
https://www.evolutamente.it/stop-ards-now-with-ascorbic-acid/
“Why Oral Ascorbic Acid Combined with IV C is the Ultimate Two-Pronged Attack That Will Turn the Tide on COVID-19 Pandemic” by Doris Loh March 25
https://www.sciencedirect.com/science/article/pii/S2213434420300153
Intravenous vitamin C for reduction of cytokines storm in acute respiratory distress syndrome
https://pubmed.ncbi.nlm.nih.gov/29684467/
Vitamin C for the Treatment of Sepsis: The Scientific Rationale – Paul E Marik – 2018 Apr 21.
https://www.youtube.com/watch?v=i4fo13Ss3VQ&feature=youtu.be
Dr Levy c19 INTERVIEW
Levy says : I consider vitamin C, magnesium, vitamin D, and vitamin K2 to be the premier, top four supplements for promoting and maintaining good health.
https://www.drbrownstein.com says “Folks, I think nebulizing hydrogen peroxide and iodine should be done on every COVID patient. It should be done on every pneumonia patient. It should be done on every influenza-suffering patient. It should be done on every patient suffering from lung problems.”
Many doctors say most lives would have been saved if they’d use hyperbaric oxygen therapy instead of intubating on ventilator. https://articles.mercola.com/sites/articles/archive/2020/05/16/hyperbaric-oxygen-therapy-for-covid-19.aspx
Ozone is probably the singular most absolute anti-pathogen. https://articles.mercola.com/sites/articles/archive/2020/05/03/ozone-therapy.aspx – Ozone Therapy for Coronavirus
Dr. Robert Rowen successfully treated ebola with ozone. He says, “.. if ozone and oxidative therapies, including Vitamin C or hydrogen peroxide or ultraviolet blood irradiation got out there, you would see a change in the landscape of medicine in this country, and it would really hurt pharma. And remember, we talked about the integration of pharma with the mass media, with the bankers and everyone else and I have no doubt that this information is being deliberately squelched. I know people, I know reporters who were trying to get the story out there and they were told by their higher ups, no go. It’s a dead story. Why? Ozone could be put into the ICUs. I have offered no expense, no cost. I don’t want to be paid for it, to go into local hospitals and bring those on in there and help. But we have a system that is so corrupt, so vile, that if it’s not FDA approved, they will let somebody die.”
https://drrowendrsu.com
https://articles.mercola.com/sites/articles/archive/2020/04/25/coronavirus-pathophysiology.aspx – How Molecular Hydrogen Can Help Your Immune System
https://articles.mercola.com/sites/articles/archive/2020/05/20/plandemic-documentary.aspx
One of Mikovits’ primary treatment recommendations for COVID-19 is interferon 1 alpha, sold under brand names such as Alferon and Roferon, to shut down the replication of RNA viruses, including retroviruses and coronaviruses.
https://articles.mercola.com/sites/articles/archive/2020/05/10/is-there-a-vaccine-for-coronavirus.aspx The Well-Known Hazards of Coronavirus Vaccines
I’ve been sending these sorts of infos out to people, but my only result seems to be a bug on my computer which denies me access to my emails. All other websites working normally except no show from hotmail. Just blank, or ignores command. flushdns did not help. Please can anyone offer any advice?
They blocked me after i sent this
https://greatgameindia.com/who-offered-20m-bribe-to-poison-covid-19-cure-madagascar-president/
Terrific to hear from someone who follows same path as me! I think one of the most serious contributing factors to the COVID deaths is the demise of the immune system, through overuse of antibiotics killing healthy microbiome, shocking obesity rates, diabetes, heart disease, etc. Healthy fit people should not get more than a mild dose of a flu. If Boris can survive….
Thanks Glenda. I agree. If you intended to devise a system to erode the populations immunity it seems lockdown would be it.
Fantastic article thanks, I had been researching the fake pandemic when I came across the Wolfgang Wodarg Council of Europe inquiry into the Fake H1N1 swine flu pandemic of 2009. The conclusions drawn by Labour mp, Paul Flynn who conducted the investigation and can be found on the COE website sound very familiar. He highlighted the convenient change in definition of a pandemic by the WHO the year before, and only after repeatedly pressing the WHO did they submit the names on The Emergency Committee. https://www.who.int/ihr/emerg_comm_members_2009/en/. The list includes Neil Ferguson, Prof Lockdown. who estimated 66000 would die in UK due to swine flu. There were 392. He has to ensure his employment at The Vaccine Impact Consortium fully funded by Bill Gates somehow. The Flynn investigation revealed 18b euros of public money was spent on vaccines, most of which were never used. Dr. Ulrich Kiel director of the WHO Collaborating Center for Epidemiology in Munster, Germany, during the hearing labelled the pandemic a hoax and said “we are witnessing a gigantic misallocation of resources in terms of public health”. The UK had 20m surplus doses from GSK, where Patrick Vallance, chief Covid adviser, was president until 2018. Meanwhile as Wodarg pointed out at the hearing, “26000 children a day are dying from avoidable diseases and hunger.” Such a pity Flynn is now deceased (Feb 19) as he no doubt would be raising Covid as another false pandemic in the UK parliament. Convenient for some!
According to the American Medical Association, the swine flu (H1N1) vaccine was associated with Guillian-Barre syndrome, a neurological disorder often resulting in paralysis and other forms of brain damage such as narcolepsy and cataplexy. The British government paid $100 million compensation for vaccine injured individuals. Source – https://blogs.timesofisrael.com/why-eu-investigated-who-for-fake-pandemic/
Wodarg has attempted to highlight the fake Covid-19 pandemic but has been discredited by the German MSM and disowned by his government as they are vaccine centric. https://www.wodarg.com/
I read your Hydroxychloriquine articles with glee, and pray mass trials will begin soon, I even admire Trump for going against Fauci and big pharma on this and taking it himself for prevention of Covid. The plant base used for Chloriquine is Artemisia which is the basis of the Madagascan drink their president has insisted the entire population take. To date there have been 12 deaths there. Many doctors have attempted to publicise the correlation between low vit D3 serum levels and Covid deaths, particularly elderly and BAME, but are being ignored by the Government and PHE. It cant be patented. https://www.bmj.com/content/369/bmj.m1548/rr-22
Thanks again for your thorough investigative journalism which I will share in the hope of waking up even 1 more person to The Truth.
Thank you Tricia for an outstanding and informative comment. Wodarg has joined the merry band of eminent scientists including Wittkowski, Ionides, Raoult and many others who have been sidelined and even accused of the cardinal sin of “conspiracy theory” for pointing out that the science governments have relied upon to inform their decision making is, well, wrong.
In truth I suspect the political decision, usually designed to benefit globalist corporations and influential foundations, comes first and then the science is either cherry picked or, in the case of Imperial College, purposefully designed to support the policy.
Hi Iain,
what a brilliant article. Thank you.
In the current situation, one is better off with increasing the ‘knowingness’ of things (the truth of a given situation) rather than getting carried with hypocritical false news/propagand/deliberate disinfo.
And your article serves as an excellent exercise to sharpen our wits.
Increasing your knowingness:
https://duckduckgo.com/?t=ffab&q=%27knowingness&iax=videos&ia=videos&iai=https%3A%2F%2Fwww.youtube.com%2Fwatch%3Fv%3D2TnULuNd5GM
Thanks Teejay. Yes I would rather face uncomfortable truth than live in comfortable ignorance.
Iain,
these 2 articles might be of interest to you:
To Test or NOT To Test? To Vaccinate or NOT To Vaccinate?
https://www.drrobertyoung.com/post/to-test-or-not-to-test-to-vaccinate-or-not-to-vaccinate?utm_campaign=4e0b3e38-5ed8-4d98-9103-680e037d3995&utm_source=so&utm_medium=mail&cid=9b3b829a-a571-4efe-9868-765326f8460a
Many thanks
First class research and very well written.
Thank you.
My pleasure. Thanks for the encouragement.